

By Lambert Strether of Corrente.
The World Health Organization (WHO) has released “Global technical consultation report on proposed terminology for pathogens that transmit through the air” (“Report”). My perspective will be institutional rather than linguistic (in that adoption of certain forms of wording, as anybody who has ever worked on a Committee knows, represents an institutional victory for one faction, and a corresponding loss for another, nostrums about “consensus” notwithstanding). While many #CovidIsAirBorne advocates (including this humble blogger) are not completely happy with some of the language, I believe that the Report represents a comprehensive technical defeat for the “droplet dogmatists” (although an incomplete institutional defeat, which sadly must take place “one funeral at a time,” though hopefully with dispatch). This may have implications for WHO’s effectiveness in the still-unreleased “Pandemic Treaty,” as we shall see).
The Report is only 33 pages long, and apparatus like Abbreviations, References, and Annexes bulks large within it. I will focus on two parts of the report: Chapter 4, “Outcomes,” which goes through the terminology of “through the air transmission,” where I will do a close reading, and Annex 5, which includes “Areas of overall general agreement” and “Areas of non-consensus and concern regarding consequences,” where I will draw out some potential implications. (As readers know, the #CovidIsAirborne network on the Twitter is incredibly diligent, skilled, and co-operative. Rather than make this post a ginormous heap of tweets from these accounts, I will list them in alpha order: @1goodtern, @DFisman, @jljcolorado (thread), @LazarusLong13, @nousaerons, and @trishgreenhalgh. If you are not following these accounts, do consider it. To them belongs the victory!
And so to excerpts from the Report, which I have helpfullly annotated in the usual fashion.
Close Reading of Chapter 4
Report, page 7:
[1] So “transmission through the air” (try saying that fast) is the supertype, and “airborne transmission” and “direct depostion” are subtypes. “Droplets” are gone (though not the dogmatists, who presumably will, at some point, be ready for their close-up[1].)
Page 8:
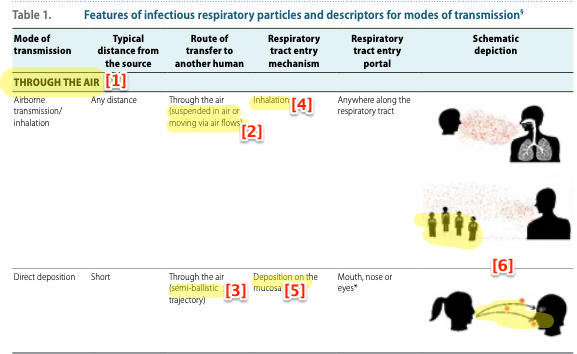
[1] Here the supertype/subtype relation described above is represented in tabular form.
[2] In other words, “moving like smoke” to “any distance.”
[3] Like droplets once were, “ballistic” (I would imagine “semi” is there because if the loogie is small enough, air currents will affect it). Importantly, we have a column for distance, but no column for size.
[4] Inhalation, by its nature, encompasses the vast majority of cases.
[5] Direct deposition, by its nature, encompasses a small minority of cases (at least for Covid). Note that Evonne Currant went through all (!) the references supporting direct depostion, and doesn’t think much of them. (The tweets aren’t threaded, so the link is to the first one. Scroll up.)
[6] The illustration shows, although the text does not, that airborne transmission implies the existence of superspreaders, while direct deposition does not.
Page 9:
[1] I think this is useful. The only similar term I can think of is virion, but that refers to the infective form of a virus outside the host cell, not encapsulated in saliva and whatever, moving “through the air.”
[2] There was an enormous literature attempting to distinguish droplets from aerosols by size. Now all that cruft is cleared away.
[3] “Puff cloud,” hoo boy. I’m sure the committee struggled with that one, but “plume” (for example) isn’t quite right, because an industrial smokestack doesn’t generally expel smoke. “Puff cloud” is getting roundly mocked:
@WHO is going cuckoo for covid puffs pic.twitter.com/D3K74eYj1o
— Sphagnum Moss (@moss_sphagnum) April 19, 2024
And critiqued:
“Puff cloud” is like a euphemism for small, easily frightened kids. But though euphemisms can make folks + comfortable, cooperative & compliant, it’s a given that they leave out important, potentially alarming or unpleasant details; that’s the point. 2 ped. dental sites, for ex: https://t.co/lKlQlCk8uo pic.twitter.com/bYuB9DntGm
— J. Offir, Ph.D. (@dontwantadothis) April 19, 2024
[4] Given this description of the “puff cloud”‘s operation, which “airborne” by itself does not include, I think it’s OK.
Page 10:
[1] Once again, “through the air” is reinforced.
[2] Personally, I’d prefer to see “airborne” as the supertype, and “direct deposition” as a subtype, with “through the air” eliminated; it makes no sense to me, as a layperson, that breathing out “smoke” and hawking a loogie are in the same conceptual bucket. Also, the symmetry between “airborne,” “waterborne,” and “bloodborne” is simple and pleasing; I don’t buy the “medium alone does not address,” because I would bet there are distinctions to be addressed between forms of water- and bloodborne transmission, too. It has occurred to me that institutional factors are at play. WHO President Tedros Ghebreyesus famously retracted “airborne” immediately after Covid team leader Mike Ryan handed him a note, and we can hardly make him (or Ryan) look bad, or all the other droplet dogmatists, for that matter. On the bright side, if “airborne” and “direct desposition” really are on a continuous spectrum from small to large — and I agree with this — then the spectrum itself needs a name: hence “through the air.”
[3] More research needed = funding. That’s good!
Page 11:
[1] Masking and ventilation now 100% legitimated as mitigation measures.
[2] Ditto the distinction between indoors and outdoors.
Page 12:
[1] Here the Committee services infection prevention and control (IPC), where Infection Control (IC) departments are very powerful in hospitals, themselves powerful at WHO. Fortunately, I have so far escaped intimate acquaintance with hospitals — and so people with experience will correct me — but from my reading I think of IC as a bureaucratic heirarchy where administrators have control over certain spaces, and adjust controls according to the risk of infection in those spaces (hence, AGP — Aerosol-Generating Procedures — but only in operating theatres). This is in fact silly, because airborne IRPs move, like smoke, through the entire facility; but there is, at present, no way to fit that ubiquity into the current heirarchy. WHO in fact reinforces this institutional structure, urging “different prevention and control measures.” So we have IC officers moving the risk knob up to 11 or down to zero, according to CDC’s horrid Green Map, putting up signs and putting out memos starting and stopping masking, all, I suppose, according to the pathogen du jour. But surely that makes no sense, giving that the Green Map lags, and, more seriously, that there may well be, in the future that awaits us, multiple airborne pathogens simultaneosly (start with Covid, RSV, and the flu, and throw in Monkeypox and H5N1). It would seem to me that excellent ventilation + respirators for all is the simplest and most robust approach, and administratively much simpler (of course, that approach isn’t a jobs guarantee for a lot of PMC, but here we are). Did I say “open rant”? Close rant.
[2] “NO suggestion” — caps in the original; typically one uses italics for emphasis, so this is really shouting — panders to IPC, as above. (One might speculate that hospitals were not willing to spend money on full “airborne precautions,” and shared their unhappiness with Mike Ryan, who then passed Tedros his note). We’ll see what CDC’s HICPAC, dominated by hospitals, makes of all this.
[3] Contradicts “NO suggestion.” This is a suggestion!
[4] A cynic might view this as allowing droplet dogmatists to slither in through the window after they’ve been thrown out the front door, but (a) without particle sizes, the droplet concept is gutted, and (b) the use case for direct depostion is mucus membranes, trivial for Covid at least, though anyone want to make book on a motivated study?
[5] Airborne transmission must always be taken into account, even if droplet transmission can be shown.
Page 13:
[1] “Inter-disciplinary research” means the days of MDs being sole authorities on matters of airborne tranmission are over (and possibly that a lot of non-interdisciplanary CDC guidance — *** cough *** Healthcare Personnel Use of N95 Respirators or Medical/Surgical Masks for Protection Against Respiratory Infections: A Systematic Review and MetaAnalysis *** cough *** — needs to be thrown out).
[2] RCT fetishists take note.
[3] Aerosol scientists must have a seat at the table.
[4] Social engineering — a nod to difficulties in mask adoption — is important.
Implications of Annex 5
Here are the “areas of non-consensus,” from pp. 32-33:
[1] As I urged above, Page 12, note 10.
[2] “If”? I didn’t know WHO didn’t support the precautionary principle….
[3] Indeed. An Annex specifying at least an approach to all this would have been helpful. Even if you had to pry the “Baggy Blues” from the dead, cold hands of IC. (This is not the first time that a public health agency has pulled its punches because of assumed costs; see CDC on school re-opening policy at NC here.)
[4] I don’t see why. I agree that the distinction between rich and poor countries is destructive. But — to pick a random example — is the West supposed to turn off its sewage treatment plants so its citizens can share cholera with the rest of the world?
A Note on Pandemic Treaty
This false post from WHO is — shamefully, if the powers-that-be at WHO could feel shame — still up:
FACT: #COVID19 is NOT airborne.
The #coronavirus is mainly transmitted through droplets generated when an infected person coughs, sneezes or speaks.
To protect yourself:-keep 1m distance from others-disinfect surfaces frequently-wash/rub your 👐-avoid touching your 👀👃👄 pic.twitter.com/fpkcpHAJx7
— World Health Organization (WHO) (@WHO) March 28, 2020
Nor has there ever been any official acknowledgement, let alone an apology, for WHO fighting the reality of airborne transmission tooth and nail for four years:
The closest we have got to an apology was @doctorsoumya “regretting”WHO’s delay in declaring SARS2 an AIRBORNE virus….
More is needed. We need an official WHO acknowledgement and investigation into what happened.
The issue is that Tedros knew from the beginning, there was no… https://t.co/EYGXb9WuF0 pic.twitter.com/KAHMqf3CFm
— John Johnston (@JOHNJOHNSTONED) April 19, 2024
Not even a “mistakes were made” non-apology!
As readers know, the “Pandemic Treaty” (though it need not be a treaty; the other options are a “regulation” and a “resolution”/”decision”) has been the source of considerable controversy (see NC here and, in part, here). KFF summarizes the state of play:
According to the latest publicly available draft text (dated 13 March), the overall objective of this new pandemic agreement is to help the world ‘prevent, prepare for and respond to pandemics.’ Among the provisions included (all of which are still being negotiated) are definitions and principles, aspirational goals for improving pandemic preparedness and response capacities, supply chain and logistics, communication, and oversight and implementation for the agreement, with some of the more contested and debated provisions being financing for pandemic preparedness and response, pathogen access and benefit sharing (PABS), intellectual property rights, technology transfer and research and development for pandemic-related products. Also a topic for debate has been the inclusion of the concept of common but differentiated responsibilities (CBDR), meant to address equity concerns by asking richer countries to take on greater obligations to address common goals in pandemic preparedness and response than poorer countries.
Since everything is still being negotiated, we don’t know very much. However, WHO possesses — or, I suppose, could be said to possess — normative authority beyond beyond legal authority. From Public Health Journal, “The normative authority of the World Health Organization“:
The WHO Constitution created a normative institution with extraordinary powers. The Constitution’s first Article enunciates a bold mission: ‘the attainment by all peoples of the highest possible level of health.’ The Preamble defines health as ‘a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.’
Article 2 grants the WHO extensive normative powers to carry out its mission, authorizing the World Health Assembly (WHA) to adopt ‘conventions, agreements and regulations, and make recommendations with respect to international health matters.’ The Organization principally exercises its normative authority through ‘soft’ power e either constitutionally authorized ‘recommendations’ or more informal action by the Assembly, Board, and/or Secretariat. The Organization rarely exerts its constitutional authority to exercise ‘hard’ power by negotiating binding international law.
The WHO’s most salient normative activity has been to create ‘soft’ standards underpinned by science, ethics, and human rights. Although not binding, soft norms are influential, particularly at the national level where they can be incorporated into legislation, regulation, or guidelines.
Please allow me to make a naive proposition: WHO could best revive its “soft power” by ‘fessing up to its mistakes, holding those who made them accountable, and in general being transparent (especially about matters of cost). I submit that such a pivot would make WHO a uniquely credible actor on the world stage. When was the last time you heard “We were wrong” from a global or national institution?
Conclusion
Returning to the linguistic mode, @BarryHunt008 provides this amusing meme:

I take the point, but I disagree. As the technical report this document is, it leaves airborne transmission advocates in a far stronger instituitional position than before, which can only be good, regardless of waffling on the Precautionary Principle, etc; a topic really not appropriate for a technical report. #CovidIsAirborne. Let’s take “Yes!” for an answer!
NOTES
[1] Here is the story of Alberta’s most notorious Professor of Medicine, droplet dogmatist John Conly, shouting down an aerosol scientist:
On the day John Conly shouted down Lidia Morawska, 3rd Apr 2020, WHO teams ALREADY KNEW the data affirming SARS2 transmission via aerosols
“Why are you asking me for evidence John? You already have the proof”
John Conly is still in post, & making decisions that affect us all https://t.co/Z0ngBbDOp9 pic.twitter.com/BWhcbus0Sp
— David R Tomlinson 🇺🇦💙 (@DRTomlinsonEP) April 20, 2024
Shouting in Committee meetings is not the done thing. Conly is so committed to the bit that he suggested vector transmission via rats for the Amoy Gardens outbreak:
Here are Conly’s rats/rat:https://t.co/BP4M9fFbwS
— Lazarus Long (@LazarusLong13) April 21, 2024
Needless to say, Conly consulted to WHO for this Report, and retains his powerful positions at WHO and elsewhere.




















{kind=link}